








Bridging the Volunteer Fulfillment Gap: Medicaid Community Engagement
Welcome back to our Community Engagement series. In the first three parts of this series, we covered the strategic vision, intelligent workflows, and IT architecture required for Medicaid community engagement. In Part 4, we step outside the government technology stack to address the physical reality of the 2027 requirements: building localized volunteer fulfillment networks and community capacity.

Under the upcoming Medicaid community engagement requirements, members will have several pathways to fulfill their obligations, including employment, job training, education, and community volunteering.
While employment or education can be documented through income verification, pay stubs or enrollment records, community volunteer fulfillment presents a distinct operational hurdle.
In this post, you’ll learn:

Why logging hours via tools like CMS Emmy is only half the battle, and why a localized resource network is required to bridge the fulfillment gap.
How to map geographic supply against member demand to ensure your program is equitable, sustainable, and legally defensible.
Strategies to prevent administrative burnout for community partners by integrating verification into their existing workflows.
The challenges with community volunteer fulfillment
Community organizations offering volunteer opportunities are highly localized and frequently operate independently. Because a cohesive network does not naturally exist, there is rarely a centralized way to identify available volunteer opportunities, seamlessly navigate members to open slots, or efficiently track and verify the hours completed.
This lack of underlying infrastructure creates a specific operational challenge for key stakeholders across the Medicaid ecosystem:

For the Medicaid Member
A member must independently locate a qualifying organization with open volunteer slots within a reasonable transit radius, secure a position, and manually track hours on paper forms. For individuals already navigating significant social barriers, this logistical complexity creates even more hurdles.
For the Managed Care Organization (MCO)
MCO care managers lack a consolidated, real-time directory of active community programs. Without visibility, they are left manually calling local food banks to find open slots, making it nearly impossible to actively navigate members to the right resources.
For the State Agency
If a state lacks a centralized view of volunteer capacity, it becomes incredibly difficult to administer the program equitably. This lack of visibility leaves agencies vulnerable to high volumes of appeals when members in rural or under-resourced areas face coverage disruptions simply because there were no local opportunities available.
Implementing a sustainable community engagement program requires solving this volunteer fulfillment gap. States and health plans must look beyond their eligibility systems and focus on how they actually connect members to the community.
Reporting vs. resourcing: Navigating federal tools
Recognizing the administrative workload of these new rules, the Centers for Medicare & Medicaid Services (CMS) released Eligibility Made Easy (Emmy), a suite of open-source tools to streamline the reporting of compliance hours.
While Emmy addresses a critical data-entry need by providing a mobile-responsive interface for beneficiaries to log activities, states must distinguish between reporting an activity and resourcing it:
- Reporting (CMS Emmy): Provides a streamlined mechanism for a member to submit their 80 hours to the state.
- Resourcing (Findhelp): Provides the network required to find those 80 hours, supplying localized directories of open volunteer shifts and adult education classes.
If states deploy reporting tools without connecting members to actual opportunities, they risk unnecessary coverage disruptions while failing to advance the core policy goals of self-sufficiency and workforce readiness.
The Findhelp standard: Community Engagement Network Adequacy
In Medicaid managed care, states and health plans rigorously monitor clinical network adequacy, ensuring sufficient primary care and specialist capacity within a reasonable distance for all members.
Community engagement introduces the parallel need for Community Engagement Network Adequacy.
To support volunteer and training requirements, states need a clear picture of local capacity. By overlaying the geographic distribution of at-risk Medicaid members with Findhelp’s network of active community programs, states and MCOs can map supply against demand.
Protecting the community ecosystem
Local food banks, shelters, and community centers are the backbone of these requirements. Yet, these organizations frequently operate at maximum capacity with limited staff.
An uncoordinated influx of individuals seeking to meet their volunteer hours risks straining these critical partners. Furthermore, if participating in a state’s Medicaid requirements means a CBO director must navigate disparate government portals or manually sign off on paper timesheets, many may simply decline to accept these volunteers.
To mitigate this systemic strain, Findhelp’s infrastructure provides CBOs with the operational tools necessary to manage their own capacity:
1
Capacity Management: Participating CBOs can set defined limits on available volunteer slots or training programs. When capacity is reached, organizations can pause incoming referrals, automatically diverting traffic to other programs with open availability.
2
Verification within Existing Workflows: As states move toward third-party verification, asking community partners to log into a separate, net-new government portal just to verify hours creates unnecessary administrative strain. By leveraging a platform that CBOs already use to manage broader social needs (like food and housing referrals), verification happens organically. When a member completes their hours, the CBO confirms participation directly within their existing Findhelp workflow, eliminating double data entry.
3
The “Closed Loop” Record: This confirmation generates a verifiable, third-party data point that can flow automatically to the MCO, the State E&E system, or seamlessly into reporting tools like CMS’s Emmy.
Proof in practice: Operationalizing network adequacy
Sourcing, vetting, and onboarding thousands of local volunteer sites is a resource-intensive undertaking. A modern infrastructure must include a pre-existing, actively managed network that captures compliance data within the exact same system used to manage a member’s broader health-related social needs (HRSN).
This concept is already solving adjacent policy challenges today. For example, certain SNAP beneficiaries in Pennsylvania face similar 80-hour-per-month work, education, or volunteer fulfillment requirements.
Faced with this fulfillment gap, the Pennsylvania Department of Human Services (DHS) leveraged PA Navigate, a statewide community information network powered by Findhelp. SNAP recipients can log into the platform they already use for social support, enter their ZIP Code, and identify local organizations with open volunteer slots.
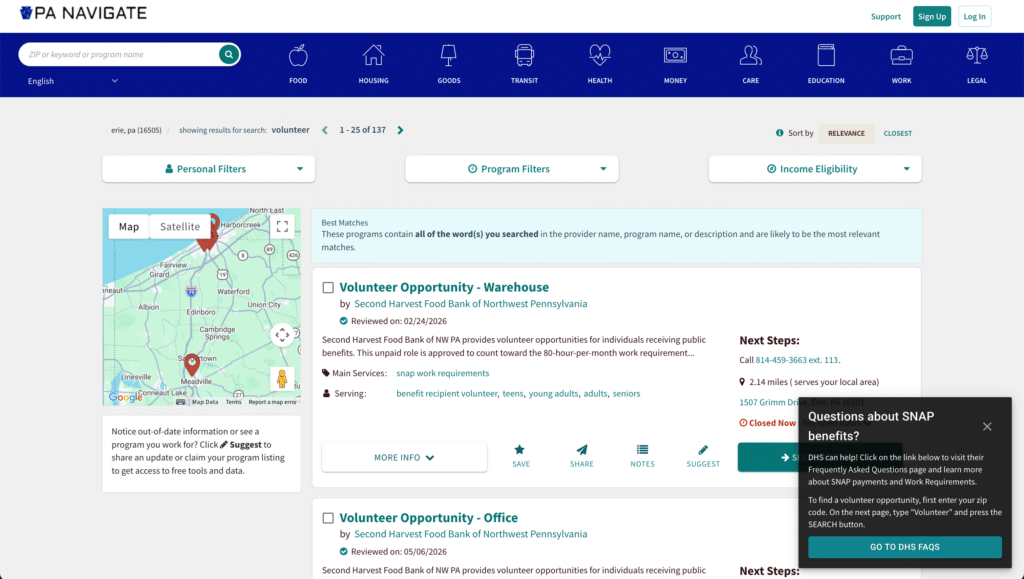
This approach gives members a clear pathway to compliance, provides the state with visibility into localized volunteer capacity, and protects CBOs from new administrative burdens.
A sustainable path forward for volunteer fulfillment
Community engagement requirements without an accurate and responsive network place a significant strain on community resources. Open-source reporting tools and modern E&E systems are essential, but they function solely as the administrative framework. The actual viability of the program depends on easily identifying and navigating the localized supply of community opportunities.
By using Findhelp to identify volunteer fulfillment opportunities, measure Community Engagement Network Adequacy, protect CBO capacity, and seamlessly integrate third-party verification into existing workflows, states can ensure that community engagement operates as a sustainable pathway to economic mobility.
What’s next?
Now that we’ve mapped the strategic vision, the workflow, the architecture, and the community network, how do we structure the underlying data to make all of this interoperable?
In Part 5, we will conclude our series by breaking down the data model that powers the future of Medicaid.