








Watch | How Trinity Health Reduced Preventable Hospitalizations by 16%
In the modern healthcare landscape, it’s increasingly clear that the majority of health-related activities happen outside the doctor’s office. Factors like access to food, housing, and social support—health-related social needs (HRSN)—can have a greater impact on well-being than clinical care alone. In a recent webinar with Becker’s Healthcare, Maureen Pike from Trinity Health and Carla Nelson from Findhelp discussed how embracing this reality helped Trinity Health achieve a 16% drop in preventable hospitalizations for its most vulnerable patients.
In this post, you’ll learn how:

Trinity Health embedded Community Health Workers (CHWs) directly into its clinical care teams to bridge the gap between healthcare and a patient’s daily life.
The program focused on reducing preventable hospitalizations, specifically for high-cost, high-need patients dually enrolled in Medicare and Medicaid.
Trinity integrated Findhelp into Epic, their electronic health record, to streamline referrals and navigation.
This initiative led to a 16% reduction in preventable hospitalizations for the target population.
The challenge: Preventable hospitalizations
Trinity Health focused on preventable hospitalizations—admissions for conditions like heart failure or diabetes that could have been managed in an outpatient setting—as a key metric. They discovered that patients dually enrolled in Medicare and Medicaid, had an avoidable hospitalization rate more than double that of the general population.

“Within this clinically integrated network, we have to look at patients’ social needs and their social circumstances and how that is affecting care plans, to be able to have their basic needs met every day… It’s not only in the value-based environment, but there’s definitely a great case for it when you’re trying to really comprehensively serve a patient and you’ve got a business model where expenses can be justified by their impact on the eventual outcome and eventual total cost of care.”
Maureen Pike, MPH, MBA, RN
Director, Clinical and Social Care Integration at Trinity Health
The strategy: Integrating social care into clinical teams
Trinity Health integrated social care directly into its care model. To address their preventable hospitalizations disparity, the system invested in an internal workforce of Community Health Workers (CHWs):
- These individuals are trained laypeople who act as a vital link between the health system and the community.
- They are part of the clinical care team, documenting in the EHR and communicating securely, but they also connect with patients in their homes and communities.
- This dual role allows them to bridge the gap between clinical needs and real-life social barriers.
“There are many ways at Trinity Health where we have formally integrated community health workers into care teams, as well as social needs screening. Even before it was a requirement from accrediting bodies or a regulatory requirement. We have institutionalized and systematized social needs screening so that we can identify those patients who have needs, and then have a workforce in place that is best suited to be working with those patients… the community health workers are a really important investment.”
Maureen Pike, MPH, MBA, RN
Director, Clinical and Social Care Integration at Trinity Health
Empowering staff with the right tools
To maximize the CHWs’ impact, Trinity Health provided them with a powerful tool: the Findhelp platform. This online network of community resources helps patients and providers find up-to-date, free, or low-cost social services by need and ZIP code.
“[Binders and pamphlets are] hard to keep up to date. And as people move on from their roles or we know there’s a big wave of retirements coming for health care professionals, that knowledge leaves with that person when you’re just counting on what’s in people’s brains or, what’s in the binder, over at the nurses’ station. But Findhelp takes all of that knowledge out of people’s brains and puts it in a searchable place, and this has been helpful on several levels. One, you know, we love to systematize. We love to scale at Trinity Health. This is scalable. This is something that can be and is available throughout our entire system. It’s integrated into our EHR.”
Maureen Pike, MPH, MBA, RN
Director, Clinical and Social Care Integration at Trinity Health
Findhelp’s integration with Trinity’s Epic EHR streamlines the referral process. When a patient’s social needs are identified during a screening, a care team member can immediately pull up a list of relevant resources and add them directly to the patient’s after-visit summary. This approach not only supports the CHWs but also enables patients to self-navigate, broadening the program’s reach.
The results: 16% decrease in preventable hospitalizations
The success of this integrated approach is visible in both the data and individual patient stories. In a four-year analysis, from July 2021 to July 2024, Trinity Health achieved a 16% decrease in preventable hospitalizations for dually-enrolled patients and a 45% reduction in health disparities between duals and the overall patient population.
Success in South Bend
Select Health and St. Joseph Health System, part of Trinity’s accountable care organization (ACO) in South Bend, Indiana, saw extraordinary results during the same four-year period:

The preventable hospitalization rate decreased 41% for duals and 15% for the overall patient population.
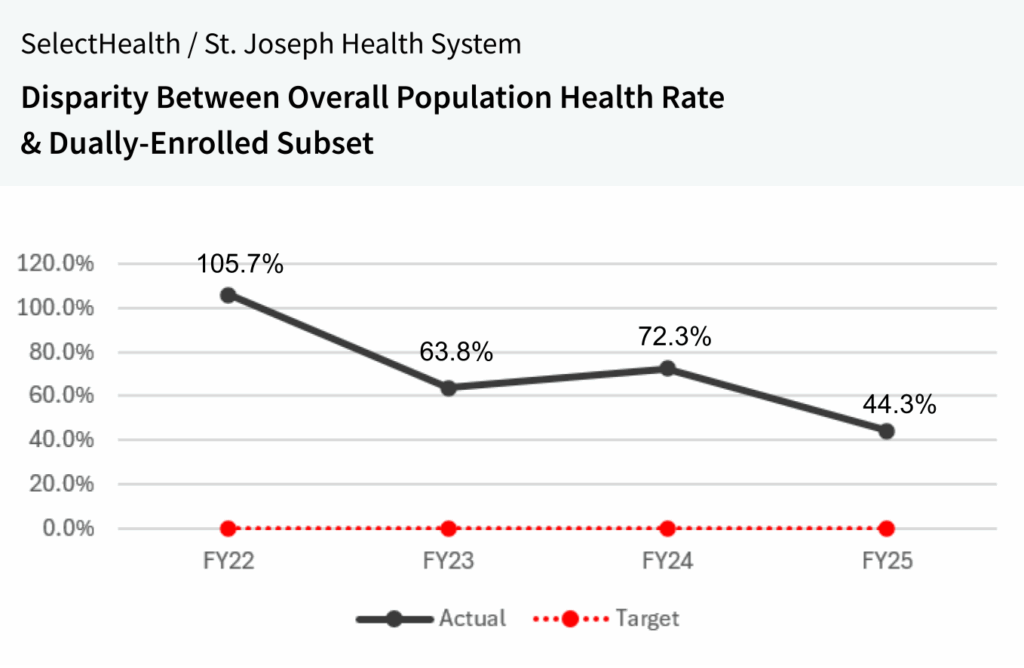
Health disparities for duals decreased by 58%.
One patient’s story: The impact of CHWs
The numbers are brought to life by stories like that of Miguel, a 49-year-old Trinity Health patient with heart failure.
- Overwhelmed and living alone, he was referred to a CHW who visited his home.
- The CHW provided him with simple tools like a scale and a pillbox.
- They also connected Miguel to more advanced services like heart-healthy meal delivery and housekeeping services.
- As a result, Miguel’s missed appointments dropped by 90%. He also enrolled in cardiac rehab and nutrition classes, regaining control of his health.
Watch: Trinity Health’s strategy & lessons learned
In a webinar with Becker’s Healthcare, Maureen Pike (Trinity Health’s Director of Social & Clinical Care Integration) and Carla Nelson (Findhelp’s Sr. Director of Healthcare and Public Policy) discussed key insights from Trinity’s approach to reducing preventable hospitalizations and health disparities:
- How to scale CHW integration across multidisciplinary care teams
- How to align clinical and social care with the right tools
- How social care platforms helped streamline referrals and close gaps
Hello, everyone. This is Moriah Mohammed with Becker’s Healthcare. Thank you for joining us for today’s webinar, what drove Tranny Health’s fourteen percent drop in preventable hospitalizations. Before we begin, I’ll walk through I’ll walk us through a few quick housekeeping instructions. We will begin today’s webinar with a presentation, and we’ll have time at the end of the hour for a question and answer session. You can submit any questions you have throughout the webinar by typing them into the q and a box you see on your screen. Today’s session is being recorded and will be available after the event. You can use the same link you used to log in to today’s webinar to access the recording. If at any time you have issues with audio or visuals, try refreshing your browser. You can also submit any technical questions into the q and a box. We are always here to help. With that, I am pleased to introduce today’s speakers, Maureen Pike, director of social and clinical care integration at Trinity Health, and Carla Nelson, senior director of health care and public policy at Findhelp. Thank you both for being here today, and I’ll now turn the floor over to you to get us started. Thank you so much. I really appreciate the introduction. As Mariah said, I’m Carla Nelson at Findhelp. We are really thrilled to be here today and really, grateful for those of you who have joined us today. Just before we get started, to give you a sense of where I’m coming from. My entire career has been focused on the intersection of health care operations and policy. I have been with Findhelp for nearing two years, helping them to navigate policy to inform Findhelp use. Before this, I spent eleven years at a hospital association focusing on population health, and I started my career with seven years on the ground running ambulatory care practices at a large health system. So all of that to say is I have a deep appreciation for the kind of work that we’re discussing today. And those of you who who are in similar positions, who have run these operations on the ground, that’s where the magic happens. So we at Findhelp are a very small part of the incredible work that Maureen and others at Trinity are leading. So, Maureen, I’m very excited to learn from you today. So welcome. Thank you for being here with us. And before we get started, how about you tell the audience a bit about yourself and your background, and then tell us a bit about Trinity Health. Thank you, Carla. I’m very happy to be with you all today. I also have spent my career at an intersection, I would say. Began as a nurse at the bedside, worked in critical care, and what I saw there and in the health care system led me more in a public health route. So I spent several years at small local nonprofit, community based organizations, and then also spent six years at the YMCA of the USA, which is the national resource office for the Y, here in our country. So I’ve gotten a lot of good community based organization experience, but it was always at the intersection of community based, you know, social services type work and formal health care delivery. And so that was a great preparation now to come into this role at Trinity Health where we’re kind of bringing those worlds together and trying to integrate it well so that we can more comprehensively care for our patient. So a little bit about Trinity Health. We are one of the largest Catholic health care systems in the nation. So we’ve got, last count, ninety three hospitals. We’re spread across sixteen states with those kind of full, health systems in local communities. We’ve got a large medical group with, over nine thousand employed physicians. And then we also own some urgent care centers, some, PACE programs, and, home care, continuing care locations. There’s a lot of variety. But what I’m gonna talk with you about today has a lot to do with what I have circled here, our integrated networks. So these are our, legal entities that are holding value based contracts with payers. And then the counterparts to those are the regional health ministries, as we call them, or regional health systems, made up of both the hospitals and the collection of ambulatory services in each of the markets and, you know, the work and the, clinical and social care services that are available through those structures. Also, I want to mention, I think a lot of the reason that this work we’re going to talk about today has been possible at Trinity Health is because our our history, and and current state as a Catholic health care system, there’s this long tradition of social awareness and social justice and the Catholic social mission. And I will say that Trinity Health really does stay true to that. And so there has been investment in having this commitment. One of our values is a commitment to people experiencing poverty and other vulnerabilities, and we believe in the dignity of every person. And so I think that is why we’ve been able to, have the investment that we have in social care and the buy in to really bring it together with our clinical care, which we’ll talk more about. And can you talk a little bit about your community health and well-being division? I would imagine that they’re a very big part of that of that, component of the mission. Yes. So, those of you who also have some of this work going on at your health systems will appreciate there are sometimes different places where this type of community health work can sit. For us at Trinity Health, it currently sits within sort of our clinical vertical, and that’s been very helpful as we have tried to, really bring that social care alongside clinical care. But we at the system office for Trinity Health, we’ve got a community health and well-being department. The focus of that department is the type of social care and addressing patient social needs that I’ll talk about today. We also do, community benefit tracking, community health needs assessment because we’re a nonprofit system. So we’re doing those requirements. Community health and well-being department. And at the system office, our team supports community health and well-being teams in each of those markets where we’ve got a local health system and a a clinically integrated network. Great. Thank you for that background. And then we’re gonna be talking a bit about preventable hospitalizations today, and we do have a very varied audience today. So let’s just level set. Can you provide some background on the preventable hospitalization measures and talk a little bit what about why they’re so important in your health system? Yes. And they are important to us. So preventable hospitalizations is a metric that has been defined by AHRQ, the Association for Healthcare Research and Quality. So it’s not our metric. It’s one that we pulled out from the But what it’s measuring is the rates of hospitalizations that occur within a defined population where the admitting diagnosis is one of a list of about dozen diagnoses where, really, that condition should have been manageable in an ambulatory setting. It should not have if it had been, you know, optimally managed, it would not have progressed to requiring a hospitalization. So, basically, basically, we look at that to say, we could have avoided this hospitalization, and we need to do some work to figure out how to do that going forward in the future. So those diagnoses, I won’t go through them all, but, several of them have to do with diabetes complications. There’s also bacterial pneumonia, urinary tract infection. The one we focused on a lot that really drives the number is heart failure. That’s the big one. So we’re really looking at it as these are events that could have been avoided, should have been avoided, and what can we do to avoid them in the future. And it’s a great score, kind of a lagging indicator to look at. We’re we’re using it within our population of patients, for whom we have value based contracts with payers. So when you’re assuming total cost of care, responsibility for a patient, this becomes a really helpful indicator of, are all our pieces and parts working together well where these patients are getting what they need? And if they progress to needing hospitalization, we gotta go look at our system and all that we have going on within our, clinically integrated networks to see how we can do better. Thank you for that level setting. We’ve talked a lot about another aspect of your organizational structure, and that is your long standing community health worker programs. And just to tie that back to the question about preventable hospitalizations, I think everyone here today knows that, what happens in community and what happens in the home and what happens in your own built environment can impact one’s health. So can you talk a little bit about the health system’s decision to invest in a community health worker program? And just tell us a little bit about how that program is organized. Yes. So we know, research has caught up with the logic around how the conditions in which you live every day and the behavioral choices that, you know, can result from those conditions have the most to do with health outcomes, even more so than clinical care. So, you know, now that we know this as an an industry, it’s kinda hard to turn a blind eye to that. We know if we really want to improve the health of a population, which is our responsibility in this value based environment and in fee for service environment too, that’s our goal. But, the value based business model is really looking at that responsibility. And so the thought was both because of our commitment to serving people experiencing poverty and other vulnerabilities and recognizing that these there can be a lot of challenges for those folks and for serving those folks, but that is what we are called here to do. We need to consider that in addition to all of the clinical services and the care coordination that’s going on, within this clinically integrated network, we have to look at patients’ social needs and their social circumstances and how that is affecting care plan, you know, to be able to have their basic needs met every day. So we do some of this work, you know, in the fee for service land as well. It’s not only in the value based environment, but there’s definitely, a great case for it when you’re trying to really comprehensively serve a patient and you’ve got a business model where, expenses can be justified by their impact on the eventual outcome and eventual total cost of care. And the logic is there to be addressing patient social. So there are many ways at Trinity Health where we have really formally integrated community health workers into care teams, as well as social needs screening. Even before it was a requirement from accrediting bodies or regulatory requirement. We have institutionalized and systematized social needs screening so that we can identify those patients who have such needs and then have a workforce that is best suited to working with those patients. And community health workers, if you’re not familiar, they are laypeople who are trained and certified to be able to come alongside a patient like a peer, particularly patients who are experiencing poverty or in these vulnerable populations where there can be a lot of mistrust with the health care system, or if not mistrust, a feeling of maybe alienation because you’re you don’t fit well into the system. You have a lot of barriers to using different parts of the system that maybe other patient populations that works great for them. There can also be sometimes intimidation or lack of good communication when you’re working with individual providers. So the community health workers are a really important investment. And at Trinity Health, we made the decision that we want internal community health workers as part of our care teams. And I kind of I always see them as sort of a a hinge where they are insiders on the care team. They are documenting in the medical record. They are able to communicate securely with all the patient’s care team. They can see all of the, you know, health care services that that patient is being provided at Trinity Health. They are on the inside of that care team. And, also they are folks who come from the community, who have a really good understanding of that community and the circumstances in which our our patients are living, and they can be that liaison out to community based organizations and social service providers and really help patients to navigate the social safety net such as it is, and also communicate that back to the the care team. So we’re really forming that bridge on both sides with good communication and good visibility into the work on both sides. So, I think that is really why the infrastructure was created and supported by our leadership and also how we’ve tried to evolve it. So there’s more I can say about the model, Carla, but I’ll I’ll see what fits best into our next topic. Yeah. Yeah. Definitely wanna hear more about the model, and do I do wanna take a moment to acknowledge that there are many models used out there for incorporating community health workers. And so we’ve seen deep partnerships with local community based organizations who actually are the employers of those community health workers. And then that health system or, you know, or hospital or health care provider is partnering very closely to determine what that management model and what that partnership model looks like to be able to best serve, serve the the people that they jointly care for. But, yeah, any other details you’d you’d like to share about the model and kind of how it’s evolved over time, would be great to share at this point. Sure. Well, I do you you call out a good a good thing there that there are a lot of different models, and there are many great community based organizations that have community health workers. And in some instances, that’s gonna be the best option for a health system might be to partner with a community based organization and utilize their community health workers. For Trinity Health, our structure and our culture, we’re we’re very much about systematizing. For instance, we have a single instance of Epic across our entire network. We’ve got, like, a couple more markets that need to roll on to that, but, that works well for us, and we’re able to make decisions about how documentation is done and, how data is obtained and all of that that applies across our entire system. We also have a largely employed provider model, and that’s not the case everywhere. So for us, we’ve got, you know, Trinity Health system, and a lot of things are standardized across our system. We’re always trying to reduce unwarranted variations in clinical care, and so we take that over to our social care. So in our culture, in our structure, it makes sense for us to have CHWs that are our employees and they’re within our care teams and, you know, utilizing those same systems. And we’ll talk about those same systems. And we’ll talk about Findhelp. That’s another important system that we use across our enterprise, but that worked well for us. And then some of the challenges that we ran into in, you know, integrating those community health workers, the work really started maybe like probably fewer than ten years ago. And we got sort of a boost during COVID because it became so clear how many people had social needs and very clear which populations were really suffering disproportionately from all the impact of COVID. So, you know, there was a lot of activity then. But since then, we’ve evolved it. And one of the important things for us was to develop our own internal training standards and a certification that we use internally because not all of our states that we are in have a state certification available for community health workers. And we knew in order to gain credibility, our CHWs don’t necessarily have degrees. That’s not a requirement. The lived experience is a requirement for a community health worker. But that’s not typically how, you know, we in the health care industry think about someone’s qualifications. And so it can be a little off putting at first. The care team’s like, who’s this person? They don’t have a license. You know, can I trust them to be a part of my patient’s care? And so building some of that structure, creating a certification that can, you know, includes continuing education requirements, we kind of mimic that type of, credential, I guess you could say, within our organization so that we could have a shorthand for all of our clinical teams that we’re trying to integrate with to let them know this is who is coming to you. This is how they’ve been trained. This is what they know how to do. These are what their competencies are, and this is how we’re maintaining and checking on that quality over time. So that’s been a big help, I think, in being able to not only standardize and and monitor quality of the work across the board, but also to be able to raise awareness and really educate, especially our clinical colleagues on who these folks are and and how they can benefit their team. Yeah. That work with the clinicians is so important also, and, you know, having them learn about what the role of a community health worker is and how they can best interact with them. So going a little bit off script here, we’d love for you to talk about, how how are those community health workers working hand in hand with the care teams, and and what did you do to train, the physicians to learn about the role and to learn about, you know, what they could do, maybe what they should not be doing? Yes. And it you know, the awareness raising and education is an ongoing process. But I would say, and I can kind of share it, I think, on my next slide here. So this gives you sort of an idea. It’s a busy slide, but it shows you how a CHW fits into a care team. And so often, especially when we’re talking about our clinically integrated networks and our value based care and care for attributed lives, the CHWs are most closely linked with the nurse care managers and the social workers who are part of those ambulatory care teams as well as ambulatory pharmacists. And so the model for that interaction has been not only, you know, knowing how to read each other’s notes in the EMR and being able to send those secure chat messages. We’ve done a lot of education on how to refer to a CHW. There’s a referral process, you know, within our EMR, and we want to keep track of those referrals. I mean, that’s one of the indicators to us that our care teams are embracing these CHWs is how many referrals are we getting from providers or, you know, other health care professionals to our our teams. And so there’s been a lot of education going to the meetings of the care managers, really doing one on one coaching in different markets where those of us from system office who support these different types of colleagues will come together and join them for a meeting and really talk about some of the best practices, the models that are working elsewhere, connect them with folks in other markets who have, know, figured something out that’s working well. And then I think it’s just just also been over time. We’ve seen it takes time for the warm up to occur. But as the CHWs start solving problems that are so painstaking to solve. I mean, navigating the social safety net is not easy. Helping patients with applications, doing the calls to find out, oh, we’re on the wait list or, you know, managing that, with all these different kind of programs. Our care managers and social workers, you know, have started to see that, like, oh, this person has the time. They get to wake up thinking about how to connect these patients to services along with the cultural brokering that they provide with the care team. And it’s work that others don’t license, you know, work for all of our professionals. So I think we try to gain the credibility by having, you know, solid training and communicating those certification requirements, but really sharing the stories and going to case review meetings together and starting to collaborate on patients, they start to see, oh, this person’s a big help to me, and we wouldn’t have been able to do this for the patient if it hadn’t been for the CHW. Providers see that too. They see you when the CHWs are solving problems for their patients who’ve got these very complicated social situations sometimes that a provider is not equipped, you know, to address. And so it gives them peace of mind to know that there’s somebody who, again, wakes up thinking about how to help patients with those problems that just befuddle us sometimes in the clinical environment because we’re not, prepared to be able to address them and navigate those community systems. Yeah. Absolutely. Thanks for diving into that. And I think as as folks, the odd the audience, as you’re thinking about what could my community health worker program look like or what does it look like today, those considerations are all very important. That physician engagement, thinking about the interaction in the context of your physician employment model, as you mentioned, Maureen. Thinking about your electronic health record and what documentation looks like. So there really is so much to consider. So I appreciate you, diving into that. And along that vein, obviously, there are a lot of tools that have had to support your efforts. And so you talked a bit about a little bit about the EHR, and you talked about, the certification. The community health workers have a really demanding role, so they are going to need, bits and pieces that will help them to manage their work and make sure their efforts are effective. So can you talk about those tools that they’ve used? Absolutely. Well, of course, the first one that I have to bring up is Findhelp, and, that would be the first one in any setting even if I weren’t talking to you right now, Carla, because it’s, I’m sure many people on the call are familiar that, you know, find help is, an online up to date database of free and reduced cost resources that you can search by need and by ZIP code. And so it’s a way to really zero in on what is available in my patient’s community. Now you have folks on the team, community health workers, social workers often who might say, I know what’s available in my community. Like, I’ve got my binder here. I’ve got all my, you know, pamphlets that maybe are ten years old, but, you know, I haven’t stopped by to get another one yet. Like, that kind of thing, it’s hard to keep up to date. And as people move on from their roles or we know there’s a big wave of retirements coming for health care professionals, that knowledge leaves with that person when you’re just counting on what’s in people’s brains or, you know, what’s in the binder, over at the nurses’ station. But Findhelp takes all of that knowledge out of people’s brains and puts it in a searchable place, and this has been helpful on several levels. One, you know, we love to systematize. We love to scale at Trinity Health. This is scalable. This is something that can be and is available throughout our entire system. It’s integrated into our EHR. It’s also available as a public facing URL or even within our, employee desktop on all of our computers, it’s accessible. So we’ve done tons of training and promotion because it helps colleagues, especially those who aren’t used to searching for you know, community resources like this. But really anybody can go in and see, is there something new? What is it that’s available near this person? And we’ve done a lot of enhancements to try to make that easy. For instance, now we have the Findhelp URL is printed on all of our after visit summaries no matter what, and that’s ambulatory and inpatient. It’s also set up in the system as some on the an audience might be aware that someone can go in within Epic, search find help, identify specific resources for a patient, and have those specific resources added to the after visit summary. And these things are so helpful because as much as a community health worker can help with a a patient with high social acuity, if you will, we don’t have enough of a workforce to help everybody who has a need. And so, you know, there’s evidence out there to show, especially with a tool like this, that somebody can self navigate, or a team member that doesn’t specialize in knowing social services can still kind of help to point the the patient in the right direction. And, having that up to date information and the ability to submit updates or submit new programs, it really sort of crowd sources that information in some ways, so that you’re not as worried, like, is my information out of date or am I missing something? It’s it’s kept up to date for you, and you can always go back to it. So, it’s been a really important tool for us. Yeah. And you mentioned two things here that I wanna dig into a little bit. One is is that self navigation. Can you talk a little bit more about what that means and and how you’ve seen that be helpful? Yes. So that would be if you are telling the patient, that the community we call it the community resource directory. That’s how we refer to to our instance of Findhelp. Being able to share a QR code on a postcard or, you know, as I mentioned, I believe the QR code is also on the after visit summary, and you let patients know. We track the number of nonemployee users, and we see it go up every year because people do go to this, and you’ll hear patients say, like, oh, wow. I just needed to know what was there. I can make phone calls. I can, you know, go to these places to see what they have to offer, but they just didn’t know what they didn’t know or how to find the information. So it’s very easy for anybody to go on the website and say what kind what you need and what your ZIP code is and find a whole list of programs and their contact information. So we’ve seen it really be, heavily used, not only by our patients, just by the public in our markets. That’s easy to use. Right. And then that’s all that’s all tying back to that mission. Right? And understanding that when you’re thinking about preventing hospitalizations and you’re thinking about addressing things in that built environment, this is a tool that that does help to to do that. And the other thing that you mentioned was integration. You’ve talked about you’ve said that, it’s integrated into your EHR. Can you just, share what that means and how that’s helped your CHW workforce? Yes. And other workforces too, but definitely our CHW. So right now, if you go into our EMR and see where the patient’s social needs screening results are. If they have a social need, then a link lights up below that where you can connect into Findhelp. Now we’re currently using native integration. We’re looking to move into launch integration for those who know what that means. But right now, when you click onto that link, there is a search box right in there within Epic without leaving the system where you can say what you need, and, the patient’s address is actually automatically populated since we have that in in the EHR. And you search just like you would on the, on the public facing website, and it will bring up the list of services. And you can click on the ones that are of interest to the patient or that you’re recommending for the patient, and it’ll pull them all into the, after visit summary. So it’s really as simple as that. There’s not much more to it, but it’s made to be, very accessible at the point where you’re identifying the patient’s social needs that you can go right into that and and help them find, at least point them in the right direction with some resources to follow-up with. Great. Thank you. So we’ve talked about your community health worker model. Right? This is the workforce that is really making a significant contribution to the successes that you’ve seen. So how are you measuring the success of these efforts? Whether that’s in the context of your, CINs or other other efforts, that you have. How are you measuring what’s going well? Yes. So definitely with the CIN, of course, you know, value based payment models always come with a lot of metrics that are being tracked, and this is one that we’re, tracking the preventable hospitalizations. But that is that is what has been elevated as a KPI. It’s on our scorecards across the organization, so there’s a lot of visibility into that rate specifically. And, certainly, I would never suggest that our CHWs are, you know, the only thing affecting that rate. There’s a lot of work going on, especially I mentioned heart failure is sort of the number one driver of that rate by far. And so there’s a lot of work going on to coordinate clinical care to connect with heart failure clinics to the PCPs and, for our pharmacists. They’re promoting guideline directed medication therapies. There’s a lot of these different pieces and parts that are happening. The community health workers are one piece of that. But an important piece, I would argue, because within the so this measure we’re applying within our Medicare shared savings program. So those are traditional Medicare patients that have been attributed to our accountable care organization. Within that population, about thirteen percent of those patients are dually enrolled in Medicaid. And school eligible or dually enrolled patients, there’s a lot of data out there nationally. It’s very clear that this is sort of a different population than those who have Medicare only. Certainly, if you qualify for Medicaid, you necessarily are much lower income or perhaps a spent down asset. So your financial status is kind of inferred from that. But we also know those patients tend to be younger. They’re more likely to be disabled. They’re more likely to report their poor health. Their costs are more than double. And this is national stats, not Trinity Health. The cost for the dually eligible population is more than double that of a Medicare only. And so our community health workers have not only been involved to kind of help round out that care that’s being provided and really bring in that socially focused piece, but we’re also able to advocate for and to focus on the health disparity that exists between our dually enrolled subset of this population and the overall population. And so there’s been this element of health equity and advocacy that has also been a piece of bringing the social care to that care team, and really being able to focus in on those patients. And it turns out that those are the highest cost patients. So, you know, it’s a population that is of interest, both for the business model and certainly just for the way that we provide care. Thanks. And we know that you’ve been tracking these measures very closely. Can you talk a little bit about how they’ve trended over time or, things that you’ve seen sort of bright spots? What what are those measures look like? Oh, yes. I I did not actually fully answer your last question now that you, state the next one. So we look at that preventable hospitalizations measure as sort of the ultimate needle that we’re trying to move. To look at within the community health worker piece of that puzzle, it has been data has been a struggle. So one of the things we we’ve always had our community health workers documenting in the EHR, but the folks that you want in those positions who are from the community, they know what it’s like to struggle and to try to navigate those social services, and perhaps, you know, have high school level education. They may not have a ton of computer skills. So imagine going from not being on commute computers very much to, like, documenting an epic. It’s a little bit mind blowing. So we’ve had to work very hard on documentation quality, which we are seeing improve, but we really need that before we can clearly say, here’s how the CHWs are impacting the clinical outcomes for x group. Right now, what we’re able to track, we have a lot of process measures, and then we’re also able to you know, like, the number of patients who are referred, the number of patients who enroll with the CHW, how long they work together, those kind of things, what what they’re working on. Our one our best indicator of success right now is we’re able to we we’ve got a part of our documentation format that looks at each individual social need that the community health worker is helping the patient with. And so we’re looking at the the success rate of when you close out the documentation on that social need, did the patient’s need get met? And right now, we’re at about seventy five percent of those social needs that CHWs are working with patients on are being resolved satisfactorily. The patient achieved their their goals as we say. So that’s our biggest indicator of success, but we have a big need and are working now with our clinical analytics and, revenue cycle performance excellence also to look at what impact are we having on specific clinical measures and also return on investment. Great. Yeah. It sounds like it it takes a village for sure. Did you wanna walk through that slide a bit? Oh, yeah. I’m sorry. That’s why I thought you might be leading up to that, as we were talking about the measures. So we have been very conservatively working on reducing preventable hospitalizations since really the, midpoint of calendar year twenty twenty one. So, for us, FYI, the fiscal year ends at the end of June every year. So, we have about four years worth of data on this preventable hospitalizations work. And so some of the the progress you’ve seen, especially in those first three years that we’re proud of, I’m gonna show you aggregate information for the system next, but first I wanted to point out one of our markets, in South Bend, Indiana. So, there’s a clinically integrated network there called SelectHealth, and we are a joint owner in that, not fully owned by Trinity Health. But we’ve also got our St. Joseph Health System that’s based out of Mishawaka, Indiana near South Bend. And so those forces combined, our community health workers from St. Joseph and the SelectHealth care managers and, you know, our medical group in that area have been working together on this. And so the purple bar that you see, I’m gonna start over on the left hand side. The solid purple bar at the top, that is the rate of preventable hospitalizations for our dually enrolled subset in this Medicare Shared Savings Program. The green solid bar below that is the overall Medicare Shared Savings Program population. So you can see how different it is. In this case, lower is better, and our purple bar is way higher than the green bar. And we started out with quite a big disparity. So if you look over on the right, this line is just showing you the disparity. So when at the end of our fiscal year twenty two, which was June of twenty twenty two, the preventable hospitalizations rate for dually enrolled patients was a hundred and five, almost a hundred and six percent higher than the overall population, so more than double. And as we’ve seen the rates go down, we see a little bit bigger of a drop in that purple bar indicating that we kinda had further to drop with our dually enrolled population, and it’s been happening. So we see kind of a a big drop over the four years, with that julie enrolled population as we see maybe a smaller drop in the overall population. But the disparity between those two groups and between those patients who are lower income and have a lot of barriers to care and are sicker because of it, you know, maybe a whole lot of reasons it’s more challenging, we want that disparity to be zero. We should be serving our patients in a way where regardless of the background you come from, you have a a same shot at a good health outcome, and that’s hard to achieve. So we’re we’re proud of that progress over on the right that shows we went from Jules having a hundred and five point seven percent higher rate. Now it’s forty four point three percent higher. So are we close to zero? No. Are we a lot closer than we were four years ago? Yes. So that and, you know, the community health workers are really the care team members that are focused on this newly enrolled population. So we certainly weren’t the only ones contributing to this, but we do think that our ability to really intentionally focus on that population and to help other care team members kind of call out and advocate for that group has been a part of the success that we see. But I do wanna share also on a system level. So, the first three years that we were doing this, we saw really great results. So if you looked at between July of twenty twenty one and June of twenty twenty four, our rate of preventable hospitalizations for those newly enrolled patients was reduced by sixteen percent. And so that was a greater drop than among the overall population, which stayed kind of steady. When you looked at the whole Medicare shared savings program, we were kind of keeping it steady throughout those years, but a significant drop for the dually enrolled. The disparity between those two groups, the health disparity reduced by almost half. So forty five percent drop or narrowing of the disparity between those two groups. And, you know, I am seeing some questions in the chat. Folks are like, okay. How did you do that? Like, what’s the connection here? And so I would say, especially looking at that newly enrolled population that that really has a lot of challenges to accessing care, and a lot of social needs, That, I think, is really a function of each the community health worker joins the care team. They start talking with care managers about, okay, which patients are we working on? Do you have our care manager, are you working with a lot of dually enrolled patients? Maybe we’ve never kinda checked that. We’ve we’ve been looking at other data to identify those patients to work with. How many of them are dually enrolled? Which of them can be referred over to a community health worker to help with some of those social needs? Are we screening for social needs among all these patients? So it’s kind of that infiltration of the social care into the existing clinical care. Another great example is, one of the other things that we’re seeing a lot of our markets do is to try to better connect these patients to heart failure clinics where they exist. And I was surprised at the amount of opportunity there was there. A heart failure clinic existed at the health system. A lot of these patients with heart failure, for whom we are responsible for total cost of care, were not connected into that that clinic. And so now, you know, that has become an intention in a lot of places to make sure that our attributed lives who have heart failure are connected in there. But it’s been in a way that community health workers are also a part of that. So both the nurse care manager and the ambulatory pharmacist and the community health worker are now building relationships with the nurses who run the heart failure clinic and saying, oh, how do we what’s our workflow for referrals here? And, hey, if you have someone in your heart failure clinic who’s not working with us, maybe they could be, you start to get those referrals flowing back and forth. So that’s sort of, a lot of how this work has evolved is having people having this additional specialty focus of social care and then just weaving it in, building those relationships, developing work flows, sharing best practices, seeing what works over time, and then just adding it to that, that picture of how we reduce preventable hospitalizations, primarily with the focus on heart failure. Yeah. And and I wanna take a a beat here just to, put a little pin on on what you said, which is, you know, just this this story about how you had this clinic available and you realize that, well, we could be using this in a different way. And I think you see that in in a lot of health systems where really this is an iterative process. This isn’t we plop in a workforce and the workforce, you know, that this community health worker workforce does it all and turns everything around. They are certainly a very impactful component, but there are so many moving parts here. I think regardless of the size of your health system, I think there are folks here that, you know, come from very from different sort of operational, areas. And so, just I I think it’s very important to acknowledge just the sheer number of moving parts and really finding those areas of opportunity within your enterprise to say, well, how can we make this piece work better, even if it’s a small piece? So really just wanted to to take a minute to to emphasize that. Thank you for sharing that story. Speaking of stories, we’ve talked about numbers and we’ve talked about what’s happened, within within your health system. And all of that is really great to see and it can tell a story of impact. At the end of the day, we’re helping human beings here. So do you have a story from a community health worker or about a particular patient that really stands out that you can share with the group just to, talk about that piece of the impact? I do. I do. I came with a story. One of our patients, Miguel, from our Saint Alphonsus Health System, which is headquartered in Boise, Idaho, and Saint Alphonsus Health Alliance is the clinically integrated network that Trinity Health owns out there. So I’ll preface this by saying one of the very specific things we did with our community health workers, knowing that heart failure was such a driver of these, measures and also knowing that, you know, as many on the call, I’m sure, understand very well, there’s a lot that somebody who has heart failure needs to do every day to keep that condition under control, like taking your weight to make sure you’re not taking on fluid, eating that low sodium, you know, diet, taking your medications as prescribed. They they sound like simple things in the care plan, but they’re not. And especially if you don’t have enough money for food every month or you can’t afford to buy a scale or you just didn’t really understand what the doctor was saying last time you were there. Maybe there’s a language barrier. Maybe it’s a health literacy, issue. It can just be overwhelming. And that’s what happened with Miguel. So Miguel is a duly enrolled patient in our he’s in our Medicare shared savings program, qualified for Medicare due to a disability. He’s only forty nine years old, and he’s enrolled in Medicaid. So he’s a dually enrolled patient. And he got this diagnosis of health failure or, I’m sorry, heart failure. Didn’t really understand it. His only kind of support system, he lived by himself, and his main support system was his mother who lived out of state and just wasn’t really there with him. And so he he was just kinda overwhelmed, didn’t really know what to do to manage this condition. So So he was referred to our community health worker who went with them. So the social care for CHF, as we call it, it’s kind of an outdated title, I guess. We don’t really say CHF as much anymore, but it had a ring to it. We trained our community health workers on what heart failure is, and those daily habits. So we use the zone sheets if folks are familiar with those. It’s like a patient education tool that kinda tells them what symptoms to watch for, when you need to go to the doctor or the ER versus, you know, kinda keep track of things at home. But there were five daily habits that folks need to get into to kinda keep that heart failure under control. And so our community health workers were trained in that and started this program where they would engage patients and go visit them in their homes and do a home assessment. So gathering a lot of information about the patient’s life and their day to day experience, they would, with the patient’s permission, they would look at their kitchen and see, you know, do you prepare your own food? What are the circumstances here? They’d be able to see if maybe patients didn’t have very much food in their cupboard. Or they would say, you know, show me how you take your medication. And so it’s not a CHW’s place to be educating on the, you know, pharmacokinetics of a drug, but they can see where the patient scores their meds. Do they have them all dumped into one container and they just, you know, take a little out every day? I mean, you see all kind of things. But because they’re in the patient’s home, they’re able to to clock these things to see where they might be able to help the patient, get to know their family if they’re there. So she our community health worker, did that with Miguel. And so she was able to help kind of with peer to peer type education on heart failure and trying to assess, like, does he kinda understand the care plan, or do I need to have his nurse care manager come and re explain some things to the provider? She was able to provide him with simple things like a scale to weigh himself every day, a pillbox to keep his meds organized, a blood pressure cuff to do self monitoring at home. And as she worked with him, as he became more educated and got these tools, Eventually, what happened with Miguel is a ninety percent decrease in his missed appointments. So he quit no showing to appointments. And there I I don’t mean that, in a perjorative way because there are lots of barriers patients can experience that would cause you not to show up at a scheduled appointment, but he began being able to keep the vast majority of his appointments, and he enrolled in cardiac rehab, and he enrolled in nutrition classes. The community health worker was also able to help him get connected to heart healthy home delivered meals and a housekeeping service to help him since he was you know, lived alone, and heart failure can make it difficult sometimes to do all that physical work of cleaning. So that that person to person connection, that ability to know what connection, that ability to know what could help him with his habits and connect him to resources that he could afford or that were, you know, free, allowed him to get his condition under control. And, you know, now he’s, well managed and set up to be able to continue following those self management habit everyday. That’s really great to hear. And I think, nothing replaces that, stepping into the home. And you talked about the I mean, I’ve I’ve heard stories myself about the shoebox of medications under the bed, bed, and and there’s just so many so many visuals and things that one might not understand without having, really having that kind of touch point with a patient. So, thank you for sharing that story about Miguel. We’re happy to hear about his successes. You’ve had a lot of successes, but nobody implements these kinds of programs without some bumps along the way. So can you talk a little bit about some of the key challenges that you and your teams experienced? Certainly. Well, one of you know, funding is always a challenge with these kind of positions. When you are focused on patients who perhaps have Medicaid or are uninsured, you know, it’s not a revenue generation opportunity even if you are billing for those things. So, it can be difficult sometimes to get buy in for maybe the CHW to patient ratio that would be ideal for providing all the services. And so a lot of our clinically integrated networks started out with maybe being willing to fund one or two community health workers. And so it started small, really had to prioritize which patients are being worked with, But really being able to gather that return on investment data and to do that in a value based context as well as a fee for service context has proven difficult for a variety of reasons. And, you know, we’re talking about a small workforce and a relatively small number of patients that they’re seeing, so it’s hard to get up on the priority list of your, you know, EMR or EHR builder teams and stuff to kinda get things tweaked the way you want. So you’re trying to make system work for you to be able to see what’s happening. But what our ideal model was was for I mentioned we have our community health and well-being department. Our preferred model is that the community health workers are employed in that department and report up to that department, but are detailed out to different care settings, including our clinically integrated networks, maybe also to provider offices, maybe also to the E. R. Or, you know, out into the community. And the reason that we do that is because we found anecdotally, over and over again, and I think there might be literature on this as well, but a lot of times our community health workers are being underutilized when they were kind of reporting up through a clinical structure. And it’s kind of it’s not a new role in the world. It’s been around in public health forever, but it’s newer in the clinical environment most places. So folks wouldn’t really know what to do with the community health worker. Again, their credentials are you know, they’re not been on the license. They don’t have these degrees necessarily. So what do we do with them? And sometimes they would end up kind of just being relegated to, like, calling patients to make appointments and things like that when really they have this whole breadth of training to be able to help address these needs that patients have. And so that’s been a real advocacy process on our part to say, within our community health and well-being department, we understand the CHW workforce. We wanna connect all of our CHWs across the system to each other so they’re not kinda isolated out on these islands and sort of not well understood or not well utilized. We wanna be able to provide them with a very solid foundation of training, of connection to peers, of, you know, folks who just understand what it is that they’re doing, so that when they go out into these other care settings, even, you know, ideally the other care settings that have the salary in their budgets to pay for this work, but we’re able to really support the workforce and strengthen them with that community health and well-being expertise that we have. So that exists in many of our markets, not everywhere. So that’s been another challenge is to kind of work out who’s in charge here, what does this person do, who gets to say what they’re doing, or what services are gonna be included, or which patients they’re working with. And I would not say that it’s a power struggle. It’s more just like sitting down to figure out the weeds. Because if you don’t do that, then things just kinda default to whatever seems easiest day to day, and it truly is often an underutilization of this workforce. So just lots of awareness raising, lots of advocacy, and then our continued challenge to get good solid data to really reflect the outcomes of the work and not just the process measures or the social needs resolution, but really the impact on other, other metrics. Great. And, you touched on this and there was an audience question. By the way, we will, turn to the audience in in just a bit. So please get your questions in, as you think of them. But there was a question here about whether or not you bill for the community health worker services. So I know it’s such a we we don’t have a ton of time, but just just a high level of how how you’ve thought about this within your health system. Absolutely. Well, the first thing I’ll say is that within our clinically integrated networks that have the value based business model, it is not our intention right now to bill for those patients. And the reason why, very, like, high level, is that you start billing for the service, it adds to the total cost of care. Same with care managers. If you start using those billing codes for care managers, it’s gonna add to the total cost of care, which, of course, is gonna go into the end of year calculation about, you know, how much shared savings were achieved. And so in that business model, it can make more sense to just pay the expense of the salary out of your expenses and have the same services offered, but not add to the total cost of care at the same time. So I get that. But I think about seventeen percent of our, you know, revenue comes from this value based world, and all the rest of our patients are in fee for service land, and we are starting to bill there. So, you know, there are a handful of states where the Medicaid program, reimburses for community health worker services. So for the past year or a little more, we’ve been billing Medicaid for community health worker services, fee for service, in Michigan and in California. Our our team in Indiana at St. Joseph, who I mentioned before, they are gearing up to bill. As I don’t have to tell this audience, billing is incredibly complicated. And so some of the most important things I would say about that is one was the idea so we know from a compliance standpoint, we need to generate charges for every patient we serve. If we’re gonna bill any payer, we’ve gotta have the paper trail to show that that’s the charge we generate for the service. It is hard to go from being a service that we don’t generate charges for at all, and the staff don’t have anything to do with, you know, payment for services with the patient or anything and to try to then get our CHWs to say, oh, you need to be checking with this patient what their insurance is, and you need to be doing charge capture as part of your documentation. And they’re terrified that patients who cannot afford it are gonna end up with a bill and, you know, god forbid, bad debt down the road because, you know, they needed our help to find food for the month, and we’re gonna charge them for that. So there’s a lot of moral distress in the work workforce around just the idea of this, but we know, you know, there’s money on the table. We’re a huge health system. We do a ton of billing. The infrastructure is there. We’ve gotta figure out how to take this work that was totally outside of that billing infrastructure and weave it in. So there’s a lot of details to that. I participated in that process at a community based organization that launched claims billing, and I thought that was hard. Doing it within a health system was actually harder because the volume is small. The reason that we’re doing it is for the sustainability of this social care work, not because it’s gonna be, like, a big cut of revenue. So you bring it to your revenue cycle folks in finance, and they’re like, why why are we doing this? Like, this is such small, but you have to look at it from the mission perspective of this is gonna be an important piece of braided funding to keep this going. And so we’ve got the Medicaid billing going. We do want to start, utilizing the community health integration and maybe principal illness navigation codes that are currently available through Medicare. But that is incident two billing, which means a provider needs to initiate it, and, you know, there’s a more sort of paperwork that needs to happen, and more parts to get together. So we are partnering with our revenue cycle, with informatics, with our medical group, with our payer strategies group that manages all those MA contracts where this may come up, to kind of get all of that built into our system. Because, again, we love to spread and scale things system wide. We’re trying to set up all the infrastructure, within our policies in general, but also within our EHR, you know, billing aspects of the EHR so that there’s one way you document it. There’s one way you you route the charges so you don’t end up charging a patient out of pocket for something that’s absurd when they need help with a basic need and kind of systematizing that. And so we we would like to launch that Medicare billing for non APM patients within the next year, and we’re working toward that. I think what I heard you say is it’s complicated. Yeah. So I’m I’m sure folks are are are feeling that too. And, the other thing to note is that on on the Medicaid side, that reimbursement very likely does not cover, a whole lot, especially when you consider the wide breadth of work that your CHWs are doing. I’m gonna actually combine, a couple of the questions that I’ve seen in in the q and a, into some something a little bit broader. Can you talk a little bit about how your CHWs interact with community based organizations and how how they might be engaging with them? Yes. So, certainly, within a hospital, you’ve got relationships with community based organizations on different levels. They might help participate in your community health needs assessment process, or you may be providing them with, you know, grants or donations, that sort of thing. What we find with the community health workers is they are on the ground. They are on the phone with these community based organizations saying, hey. I have this patient who needs x. Like, do you have room for them in your program or whatever? So they are building the really person to person sort of operational relationships. And just earlier today, we had a system wide CHW appreciation event, and heard some great examples where you’ve got your CHWs working with their assigned patients, but then they’ll also go and and partner with a local organization that they work with every day to organize a clothing drive or, you know, to, start a food box program. And so you build on those relationships of, like, referred patients to see what our shared patients and clients community really needs and then figure out, like, how to do some of that outreach and some of that program development at the same time that they’re, you know, caring for the patients that come to them through Trinity Health. So those relationships are really important from sort of a bottom up, and then it can complement the more top down relationship that might have to do with, like, providing donations to that organization or, you know, including them in the CHNA. Great. So we are we are nearing the end of our time. I have one more sort of closing question to ask. And for those of you who did submit questions, thank you so much. We have these for afterwards, and we will respond to your questions. So, please don’t think they’ll go unanswered. But just as a closing question, we have an audience full of health systems and health care providers today. So what’s the one piece of advice that you would give to those programs that are looking to either start or scale their CHW programs to make the kind of impact that you’ve seen? The biggest thing I would say or would recommend is don’t put the CHWs in a silo. That can be really easy to do because sometimes a lot of times they are grant funded or maybe the impetus came from a a community need versus, like, a clinical need. And so it it can be really easy for this work to just kind of be off alone on the side. And we have seen such benefit from being very intentional about integrating it with the care team and making them a part of the way that we provide care for patients in general and doing that sort of in a system wide somewhat standardized way. So I believe, like, you can’t grow or scale this and you can’t make your biggest impact if the CHWs are kinda off by themselves. And maybe it starts that way, but I personally feel like a great goal is to just try to get it out in the open and integrated into the way that we provide care for patients. Here it is. Is. Yep. That’s that’s great advice, and it sounds like you have done a lot over the CHW implementation timeline, to really you and the team, have really done, put forth a a significant effort to do that. So we are nearing the the top of the hour. I wanna thank you so much, Maureen, for sharing the work that you and for others at Trinity Health have done. For the audience, I hope that you’ve been able to to learn from this and have, found some takeaways that will help the implementation or scaling of your own programs. And at this point, I will turn it back over to Mariah to close this out for the afternoon. Thank you. Perfect. Thank you so much. That is all the time we have for today. So, again, I wanna thank both of you for an excellent presentation as well as Findhelp for sponsoring today’s webinar. Thank you all for joining us, and we hope you have a wonderful rest of your day. Yeah.
The Road Ahead
While Trinity Health has seen significant success, the work isn’t without its challenges. Funding the CHW workforce and integrating their efforts seamlessly with existing clinical workflows remain key hurdles. The system is also working to navigate the complexities of billing for CHW services to ensure the program’s long-term sustainability.
For other healthcare organizations looking to replicate this success, the advice is simple: don’t put CHWs in a silo. By intentionally integrating them into the care team and leveraging technology to empower their work, health systems can address the full spectrum of patient needs. Make a measurable impact on health outcomes while lowering cost of care with Findhelp.
