








Watch | How Trinity Health Reduced Preventable Hospitalizations by 16%
In the modern healthcare landscape, it’s increasingly clear that the majority of health-related activities happen outside the doctor’s office. Factors like access to food, housing, and social support—health-related social needs (HRSN)—can have a greater impact on well-being than clinical care alone. In a recent webinar with Becker’s Healthcare, Maureen Pike from Trinity Health and Carla Nelson from Findhelp discussed how embracing this reality helped Trinity Health achieve a 16% drop in preventable hospitalizations for its most vulnerable patients.
In this post, you’ll learn how:

Trinity Health embedded Community Health Workers (CHWs) directly into its clinical care teams to bridge the gap between healthcare and a patient’s daily life.
The program focused on reducing preventable hospitalizations, specifically for high-cost, high-need patients dually enrolled in Medicare and Medicaid.
Trinity integrated Findhelp into Epic, their electronic health record, to streamline referrals and navigation.
This initiative led to a 16% reduction in preventable hospitalizations for the target population.
The challenge: Preventable hospitalizations
Trinity Health focused on preventable hospitalizations—admissions for conditions like heart failure or diabetes that could have been managed in an outpatient setting—as a key metric. They discovered that patients dually enrolled in Medicare and Medicaid, had an avoidable hospitalization rate more than double that of the general population.

“Within this clinically integrated network, we have to look at patients’ social needs and their social circumstances and how that is affecting care plans, to be able to have their basic needs met every day… It’s not only in the value-based environment, but there’s definitely a great case for it when you’re trying to really comprehensively serve a patient and you’ve got a business model where expenses can be justified by their impact on the eventual outcome and eventual total cost of care.”
Maureen Pike, MPH, MBA, RN
Director, Clinical and Social Care Integration at Trinity Health
The strategy: Integrating social care into clinical teams
Trinity Health integrated social care directly into its care model. To address their preventable hospitalizations disparity, the system invested in an internal workforce of Community Health Workers (CHWs):
- These individuals are trained laypeople who act as a vital link between the health system and the community.
- They are part of the clinical care team, documenting in the EHR and communicating securely, but they also connect with patients in their homes and communities.
- This dual role allows them to bridge the gap between clinical needs and real-life social barriers.
“There are many ways at Trinity Health where we have formally integrated community health workers into care teams, as well as social needs screening. Even before it was a requirement from accrediting bodies or a regulatory requirement. We have institutionalized and systematized social needs screening so that we can identify those patients who have needs, and then have a workforce in place that is best suited to be working with those patients… the community health workers are a really important investment.”
Maureen Pike, MPH, MBA, RN
Director, Clinical and Social Care Integration at Trinity Health
Empowering staff with the right tools
To maximize the CHWs’ impact, Trinity Health provided them with a powerful tool: the Findhelp platform. This online network of community resources helps patients and providers find up-to-date, free, or low-cost social services by need and ZIP code.
“[Binders and pamphlets are] hard to keep up to date. And as people move on from their roles or we know there’s a big wave of retirements coming for health care professionals, that knowledge leaves with that person when you’re just counting on what’s in people’s brains or, what’s in the binder, over at the nurses’ station. But Findhelp takes all of that knowledge out of people’s brains and puts it in a searchable place, and this has been helpful on several levels. One, you know, we love to systematize. We love to scale at Trinity Health. This is scalable. This is something that can be and is available throughout our entire system. It’s integrated into our EHR.”
Maureen Pike, MPH, MBA, RN
Director, Clinical and Social Care Integration at Trinity Health
Findhelp’s integration with Trinity’s Epic EHR streamlines the referral process. When a patient’s social needs are identified during a screening, a care team member can immediately pull up a list of relevant resources and add them directly to the patient’s after-visit summary. This approach not only supports the CHWs but also enables patients to self-navigate, broadening the program’s reach.
The results: 16% decrease in preventable hospitalizations
The success of this integrated approach is visible in both the data and individual patient stories. In a four-year analysis, from July 2021 to July 2024, Trinity Health achieved a 16% decrease in preventable hospitalizations for dually-enrolled patients and a 45% reduction in health disparities between duals and the overall patient population.
Success in South Bend
Select Health and St. Joseph Health System, part of Trinity’s accountable care organization (ACO) in South Bend, Indiana, saw extraordinary results during the same four-year period:

The preventable hospitalization rate decreased 41% for duals and 15% for the overall patient population.
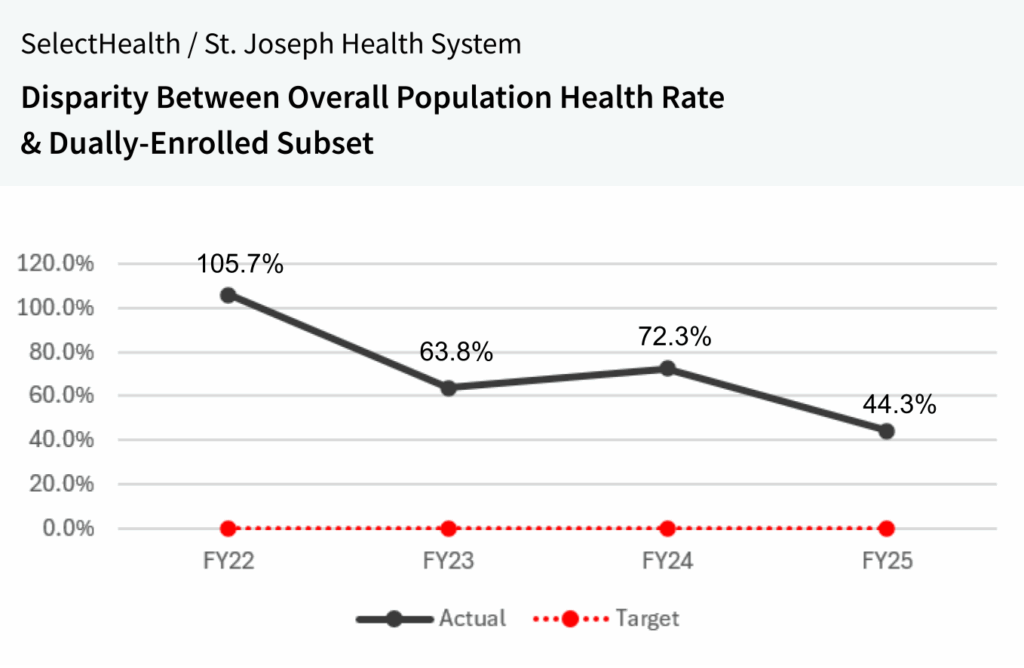
Health disparities for duals decreased by 58%.
One patient’s story: The impact of CHWs
The numbers are brought to life by stories like that of Miguel, a 49-year-old Trinity Health patient with heart failure.
- Overwhelmed and living alone, he was referred to a CHW who visited his home.
- The CHW provided him with simple tools like a scale and a pillbox.
- They also connected Miguel to more advanced services like heart-healthy meal delivery and housekeeping services.
- As a result, Miguel’s missed appointments dropped by 90%. He also enrolled in cardiac rehab and nutrition classes, regaining control of his health.
Watch: Trinity Health’s strategy & lessons learned
In a webinar with Becker’s Healthcare, Maureen Pike (Trinity Health’s Director of Social & Clinical Care Integration) and Carla Nelson (Findhelp’s Sr. Director of Healthcare and Public Policy) discussed key insights from Trinity’s approach to reducing preventable hospitalizations and health disparities:
- How to scale CHW integration across multidisciplinary care teams
- How to align clinical and social care with the right tools
- How social care platforms helped streamline referrals and close gaps
The Road Ahead
While Trinity Health has seen significant success, the work isn’t without its challenges. Funding the CHW workforce and integrating their efforts seamlessly with existing clinical workflows remain key hurdles. The system is also working to navigate the complexities of billing for CHW services to ensure the program’s long-term sustainability.
For other healthcare organizations looking to replicate this success, the advice is simple: don’t put CHWs in a silo. By intentionally integrating them into the care team and leveraging technology to empower their work, health systems can address the full spectrum of patient needs. Make a measurable impact on health outcomes while lowering cost of care with Findhelp.
